Hysterectomy
Expected length of hospital stay = three to four days
Our expectations
Prior to discharge:
- You will be able to attend to your daily needs independently.
- Your wound will be free from infection.
- You will be tolerating your usual diet.
- Your pain will be controlled with oral analgesia (pain relief).
Preadmission information
 Prior to your admission to hospital, you will be provided with a preadmission form. Please complete this form and return to the hopsital as soon as possible. Please provide as much information as possible. If you currently use a CPAP machine, please ensure that you bring this to hospital with you.
Prior to your admission to hospital, you will be provided with a preadmission form. Please complete this form and return to the hopsital as soon as possible. Please provide as much information as possible. If you currently use a CPAP machine, please ensure that you bring this to hospital with you.
Day of admission and surgery
Admission
On admission you will be taken to the ward.
You will be prepared for surgery and will be asked to sign your carepath to acknowledge your understanding and involvement of your daily care.
You will have an armband applied which will stay on for the duration of your stay for identification and safety reasons. From the ward you will be transferred to theatre.
A safe is provided in the cupboard of your post-op room to store any valuables you have brought to hospital. It is highly recommended that you leave your valuables at home for safety and security purposes.
Discharge planning
You can expect to be in hospital for three to four days or until you have met the expected outcomes for your procedure. Your nurse will discuss with you any needs that you may have following your discharge home (such as home help, blue nurses, etc.).
Please inform staff if you are currently using a community service, i.e. Blue Nurses.
Teaching and emotional support
Your nurse will explain to you the pre-op/surgical/post-op routine.
Any questions you may have in regards to your surgery or recovery will be answered.
If you would like pastoral care to visit you, please let the staff know and this can be arranged.
Following your operation you will be transferred to the recovery room where you will be observed closely for approximately 30 minutes. You will then be transferred back to your room on your bed once you are fully awake and stable.
Your physiotherapist will visit to explain exercises that will help with your post-op recovery.
Deep breathing, coughing and leg exercises are important for you to do while you are resting in bed after your surgery. These exercises help your circulation and prevent the possibility of clots forming in your veins.
To facilitate the deep breathing and coughing, a device known as a TRI-FLO may be given to you.
Deep breathing and leg exercises
Once each hour take five or six deep, slow breaths—relax your shoulders as you breathe out. Bend ankles up and down 10 times every 30 minutes.
Supporting your wound when coughing, sneezing or vomiting
 Sit forward in a chair if possible. If in bed, bend your knees up. Place both hands over your wound, with your forearms resting firmly across the abdomen. It may help you to use a pillow across your abdomen as you cough, sneeze or vomit.
Sit forward in a chair if possible. If in bed, bend your knees up. Place both hands over your wound, with your forearms resting firmly across the abdomen. It may help you to use a pillow across your abdomen as you cough, sneeze or vomit.
Mobilising correctly using your deep abdominal muscles
When you move from sitting to standing, and when you walk, try to gently activate your deep abdominal muscles. Gently draw in the abdominal muscles below your underwear. Placing your hands on your lower abdomen beneath your navel will help you to check the activity of these muscles.
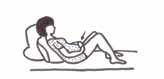
Moving in bed correctly
Slide one heel at a time along the bed towards your buttocks to bend both your knees. Keep your head flat on the pillow. Lift your bottom off the bed as you push through your heels and elbows to move yourself up the bed.
Positioning yourself to avoid straining your repair
The diagram to the right shows the correct position and technique to use at the toilet to avoid straining.
When going to the toilet, remember to keep the curve in your back as you lean forward at the hips. Lean your forearms or hands onto your knees (refer to picture on right).
Tests and procedures
Any blood tests, X-rays, ECG or other procedures that your surgeon may have ordered for you will be taken care of before you come to hospital or soon after your arrival.
Consults
Your surgeon may visit and discuss your surgical procedure.
Your anaesthetist may also visit. They will also discuss your anaesthetic and pain relief following surgery. It is important that you raise any concerns with them.
A pharmacist may visit with you. You may ask them any questions about your medications.
If you have any family or significant other who you would like the surgeon to speak with after the operation, this will be noted and they can wait in your room or a waiting area. If required, your surgeon can telephone them at home or work to update them on your condition. Please provide the nurse with the relevant telephone numbers.
Hygiene
If you are having abdominal surgery you will be required to have your pubic hair clipped.
Once you have showered (at home or on admission) you will be required to dress in a theatre gown and some paper pants in preparation for your surgery. Apart from your wedding band, no jewellery or metal is to be worn to theatre. Some tape will be wrapped around your wedding band to cover it.
After you return to the ward you will be given an assisted wash and be dressed in a clean gown.
Mobility
Immediately following surgery you will be resting in bed.
You will be encouraged to practice your post-op deep breathing and circulation exercises.
Nutrition
It is necessary that you have nothing to eat or drink for six hours before the operation. Following surgery you may have small sips of water or ice to suck on. You will also be given fluids via your I.V. drip.
Elimination
On admission you may be asked for a urine sample for testing. You may require a small enema if your bowels have not opened. After surgery you will have a catheter in place to drain urine from your bladder.
Observations
On admission your nurse will take your observations (e.g. temperature, pulse, blood pressure and weight.)
After surgery the nurse will observe your vital signs for several hours. These observations will become less frequent as you stabilise post-op.
Your wound, dressing and vaginal discharge will also be observed. You may return from your operation with a vaginal pack. This will remain in place until post-op day one.
Medications
The nurse will give you your usual medications today, unless otherwise indicated.
The anaesthetist may discuss with you the possible need for a “pre-med” before the operation.
During surgery you will receive an anti-inflammatory suppository. This will help reduce pain and inflammation in your abdomen and pelvis.
Following surgery you will have an I.V. drip to maintain your fluid intake, pain relief and antibiotic coverage during your post-op period.
You must let your nurse know if you have any pain or nausea, as your medications can be adjusted accordingly.
Your pain relief may be administered via a device call Patient Controlled Analgesia (PCA). This device (as the name suggests) allows you to control your own pain relief. The dose of the drug is set by the anaesthetist and you are given a control button that is attached to a pump containing pain relieving medication. When you press the button, a small amount of medication is delivered into the I.V. drip in your arm. There are safety mechanisms in the pump that are set to ensure that the medication has time to work before a further dose is given. If the button is pressed again within this short time, no further medication is delivered. As you are the one who can feel the discomfort, you should be the only one to push the button. It is unsafe for your family or visitors to push it instead. The PCA is usually removed the day after your operation and you will continue on oral medications, e.g. paracetamol with or without Codeine.
Following surgery you may have oxygen in place via a mask or nasal prongs. This will be removed in time, according to your observations.
You may need a special injection daily to thin your blood and prevent clotting (e.g. Clexane) if your surgeon orders one.
Treatments
You will be measured for anti-embolic stockings (TEDS) and will need to have these put on prior to going to theatre.
A sequenced pressure device (SCDs) will be applied to both your legs before surgery. This device massages your legs, stimulating the circulation of your blood from your legs back to your heart, while you are immobile, reducing the risk of clot formation.
You may require a pubic hair clip pre-operatively, if ordered by your Doctor.
Phase one - post-op
Phase one consists of day one post-operatively and any days following where you are still needing to be cared for at this level. You will progress to phase two when all outcomes for phase one have been reached.
Outcomes to be reached in phase one:
- mobilise short distances
- tolerate clear fluids and progress to light diet
- I.V. therapy to be removed
- catheter to be removed and trial of void commenced
- drain to be removed
- pain will be controlled with oral medication
- your vaginal discharge will be minimal
- your pain is managed on oral medication.
Consults
Your surgeon will visit with you and discuss your operation.
Your anaesthetist may also visit to check your progress.
The pharmacist may also visit to check your medication supply.
The physiotherapist may also visit with you.
Discharge planning
Your nurse will continue to discuss with you any needs that you may have following your discharge home.
Teaching and emotional support
A member of our pastoral care team may visit you. A nurse will discuss this booklet with you and ensure you understand your path of care.
Tests and procedures
You may have a blood test checking the Haemoglobin (iron) level of your blood.
Mobility
You are encouraged to increase your mobility as ordered by your doctor. The physiotherapist and nurse will assist you to mobilise a short distance. Your mobility level will depend on when you had your operation. If you had a morning operation—you will be encouraged to mobilise this morning. If you had an afternoon operation—you may be advised to take it a little slower and not mobilise until the afternoon of day one post-op. While resting in bed remember to do your exercises regularly.
Hygiene
You will be given assistance with showering and other hygiene needs.
Nutrition
You may have clear fluids progressing to a light diet as tolerated. A record will be kept of your oral fluid intake.
When your catheter is removed
Each time you want to pass urine please notify your nurse. It is important for your nurse to measure the amount of urine passed and then scan your bladder with an ultrasound device. This is called ‘Trial of Void’ and is done to ensure your bladder is emptying sufficiently.
Continence state
Your nurse will assist you with your toileting needs. The amount of urine you pass will be measured.
If you have a catheter in your bladder this will be removed during this phase.
Observations
Your temperature, pulse, respirations and blood pressure will continue to be monitored regularly.
Your vaginal discharge will be checked regularly. It is important to inform your nurse if the bleeding becomes bright and heavy.
If you have an abdominal wound, your wound, dressing and drains will be monitored regularly. Your drains are usually removed after 24 hours following surgery.
Medication
Your I.V. drip may be removed. This is determined by the completion of the antibiotics, whether you are tolerating oral fluids and the result of the Haemoglobin blood test.
You will be given your regular medications today. If you have any pain it will be controlled with oral analgesia. Remember to let your nurse know if you have any pain. You may be troubled with wind pain.
Treatments
You need to continue to wear your stockings as ordered.
The SCDs will be removed when you are able to walk around.
You will be encouraged to perform your deep breathing, coughing and leg exercises while resting in bed. You will be reminded to use the information provided by your physiotherapist.
Phase two - pos-top
Phase one consists of achieving phase one goals—this could be as early as day two. You will be ready for discharge phase when you have achieved all goals of phase two.
Outcome goals to be reached in phase two:
- increase mobilisation—sitting out of bed for meals and achieve four walks
- you are able to shower independently
- you will be eating foods and fluids you desire
- you will be passing urine normally
- your vaginal discharge will be scant
- your wound and drain site will be clean and dry
- your observations are within the normal limits
- your pain is managed with oral analgesia.
Teaching and emotional support
Your nurse will discuss with you this patient information booklet and answer any questions you may have.
A member of the pastoral care team may visit you.
Consults
Your surgeon will visit you and your physiotherapist (if applicable) will also continue to see you.
Mobility
You will be encouraged to sit out of bed for meals and be encouraged to take four walks today with the assistance of your nurse or physiotherapist if required. You will be encouraged to perform your deep breathing, coughing and leg exercises while resting in bed.
You will be reminded to use the information provided by your physiotherapist.
Hygiene
You are free to shower independently. Assistance will be given if needed.
Nutrition
You may increase your diet from a ‘light diet’ to eating food as you desire.
Continence state
If you had a catheter in place post-operatively:
It is expected that you will be passing urine normally by this phase.
Please notify your nursing staff if you are:
- having difficulty passing urine
- passing urine frequently
- experiencing pain or burning when you pass urine.
A medication may be ordered to help you move your bowels if you are having difficulty.
Observations
Your temperature, pulse, respirations and blood pressure will be monitored regularly.
You will be asked if you have any vaginal discharge.
If you have had abdominal surgery your wound dressing and drain site will be monitored regularly.
Medications
You will be given your regular medications plus any required for pain relief. Please let the nurses know when you have pain.
Treatments
Continue to wear your stockings.
Discharge planning
Your progress will be reviewed and it will be determined whether you are:
- ready for discharge home
- require ongoing hospital care.
If you are ready to go home your discharge summary will be faxed to your GP (if GP fax number provided) so they are aware of what care you received whilst in hospital.
Day of discharge
Consults
Your Surgeon will visit you before you are discharged.
Mobility and activities of daily living
You are independent with your walking and showering. At home mobilise around the house and yard initially, then go for short walks. Aim to gradually increase your activity every day. By four weeks you should be fully mobile.
Your bowel and bladder should now be functioning normally.
Nutrition
You may have foods and fluids you desire. A diet that promotes tissue healing, including protein, iron and vitamin C is recommended. A high fibre diet along with two to three litres of fluid each day will encourage regularity.
Observations
Your temperature, pulse, respirations and blood pressure will be monitored prior to your discharge.
The condition of your wound or dressing will also be noted prior to your discharge. Your vaginal discharge will also be noted.
Medications
You will continue to take your regular medications. Tablets are available to you if you experience any pain.
Treatments
If your dressing is removed, you may leave your wound exposed. If your dressing is intact, instructions will be given to you as to when you can remove your dressing.
You will need to continue to wear your stockings—especially overnight—for one to two weeks.
Discharge planning
Your nurse will give you a discharge advice form and discuss it with you.
It is preferable that you arrange to be ready for discharge by approximately 10 am.
What to expect
- You may have a blood stained vaginal discharge. This should be lighter than a normal period and should settle within a fortnight.
- You may feel fatigued.
- You may need to take some simple analgesia for pain/discomfort, especially on waking and settling at night.
What to avoid
- For the first two to three weeks lift nothing greater than 2 kg. Increase gently as tolerated over six weeks.
- It will take about three weeks before you should drive a car. Only when you know you can act confidently with emergency breaking should you attempt driving the car. Prior to driving please check your Car Insurance Policy to see if you are covered.
- Avoid straining when opening your bowels. Avoid constipation by eating a diet high in fibre and drinking two to three litres of fluid a day.
- Avoid inserting anything into the vagina for six to eight weeks to allow time for healing to take place.
When to notify your doctor
- if your wound becomes red or inflamed or discharge increases
- f you have heavy vaginal bleeding—heavier than a normal period
- if you develop a fever (temperature above 38 °C)
- if you have pain that is not relieved by simple analgesia
Please continue your daily exercise program as per your physiotherapy instruction sheet.
Mater Private Hospital Redland
Weippin Street, Cleveland, Q, 4163
Reception: 07 3163 7444
Visiting hours—10 am to 8 pm (rest period—1 pm to 3 pm)
Acknowledgments
Staff of Mater Private Hospital Redland & EMC@M Hysterectomy Working Party Exercise Graphics courtesy of Mater Women’s Health Physiotherapy & Physio Tools © Milliman Care Guidelines: Inpatient and surgical Care/Home Care, 12th Edition, 2008, Milliman USA, Inc.
© 2010 Mater Misericordiae Ltd. ACN 096 708 922
Mater acknowledges consumer consultation in the development of this patient information.
Mater Doc Num: PI-CLN-460013
Last modified 09/8/2017.
Consumers were consulted in the development of this patient information.
Last consumer engagement date: 28/2/2014
For further translated health information, you can visit healthtranslations.vic.gov.au/ supported by the Victorian Department of Health and Human Services that offers a range of patient information in multiple languages.