High Tibial Osteotomy
Welcome
At Mater we understand that being in hospital can be a very stressful experience. This booklet aims to alleviate some of your concerns in keeping with our Mission to offer compassionate, quality care that promotes dignity while responding to patients’ needs. It explains briefly the events that may occur during your visit and the things to expect when you are discharged from the hospital.
It is, however, only a guideline as each person may require differing treatments.
If you have any questions about your treatment please ask your doctor or nurse.
Our pastoral care team offers a caring support network to all patients. The dedicated members of this team will visit you during your stay and are available at your request to discuss any anxieties or problems that you may have.
High tibial osteotomy
High tibial osteotomy is a surgical procedure to realign the leg and reduce the pain you have from your knee by transferring the body weight to the preserved normal outside of the knee. This procedure does not return the knee to normal. However, it prolongs the life of a damaged knee, helps relieve pain in the knee and delays the need for a total knee replacement.
A triangular wedge of bone is taken from the outer side of the tibia (the bone beneath the knee). This procedure does not return the knee to normal. However, it prolongs the life of a damaged knee, helps relieve pain in the knee and delays the need for a total knee replacement.
- You will have a curved scar about 10 centimetres in length along on the outside of your knee.
- Your leg may be shorter by up to one centimetre. This is unlikely to be noticeable.
- Your leg may appear to have a degree of ‘knocked knee’.
- The surgery is done to correct the alignment of the knee not to correct instability of the knee but this may also occur as a secondary benefit.
The two figures below show you before surgery (figure 4) and after surgery (figure 5).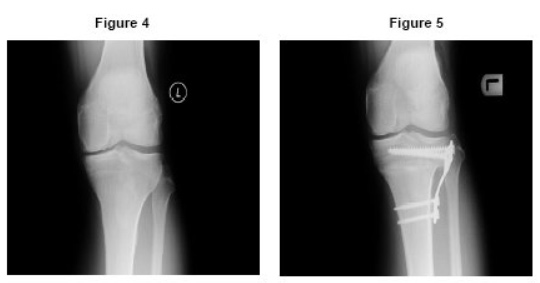
What happens during high tibial osteotomy surgery?
The “tibia” is the shin bone. In a high tibial osteotomy the bone of the upper tibia is
cut and repositioned to realign the leg. This reduces the pain that you experience in
your knee by taking pressure off the damaged joint surface. A triangular wedge of
bone is taken from the outer side of the tibia (the bone beneath the knee).
What things do I need to do to be ready for surgery?
You will have received instructions from your doctor and the pre-admission clinic.
The Clinical Nurse Consultant will call you three days from before your surgery
to ensure you are on track with your preparations for surgery.
Please follow those instructions and complete the My checklist to be ready for
surgery.
Having your home prepared before you have your operation will make things easier
when you return home after your operation. The following points are suggestions that
can help you with this:
- walkways (to be clear of furniture, loose mats or rugs, cords or leads)
- shower, bath and toilet access and safety
- kitchen layout (re-arranging kitchen cupboards may be necessary to avoid bending).
Preparing meals in advance and freezing them, or buying frozen dinners will help
make meal preparation easier when you return home. You will need to organise
family, friends or neighbours to help with the housework, shopping, driving or
providing light assistance with showering, dressing and putting on and taking off
the stockings required to be worn for six weeks after your operation.
Please complete the 'My checklist to be ready for surgery'.
What can I expect after my operation
Operation and recovery - Your operation will usually take between one to two hours.
You will then remain in the recovery area until you are awake enough to return to the ward. This may take up to three hours.
Lines and drains - When you return to your ward you may still need oxygen, will have IV lines for fluid and pain medication and you may have a catheter to help keep your bladder empty until you are able to manage getting up to go the toilet.
These will be removed gradually from day 1 following your surgery.
Diet - If you eat and drink normally straight after your operation it may cause you to feel sick. Eating and drinking small amounts slowly will help to prevent this.
You should be eating and drinking normally by day 1 following your operation.
Pain - It is normal to have some pain and discomfort after your surgery. However, it is important that your pain is controlled so you are able to cough, breathe deeply and do your exercises.
Please let someone know about your pain so it can be treated and managed.
Infection control - Every effort will be made to prevent infection. Hand hygiene is essential when recovering from this surgery. Please wash your hands regularly.
Your doctor may order antibiotics to also help prevent infections.
Blood clot prevention - To help prevent blood clots forming in your legs (thromboembolism) your doctor may request that you wear white compression stockings on your un-operated leg.
If your doctor has ordered this stocking it can be removed for your shower and put back on afterwards. You will need to wear the stockings for six weeks after your operation. Non-slip socks will also be provided. You can wear these or appropriate footwear
over your stockings.
You will have blood-thinning medication which may continue when you go home. If your doctor orders this, your nurse will provide education for you or your carer to manage when
you go home.
Mobilising and exercising - You will have a knee immobilizer in place at all times.
The day following your surgery specific instructions and assistance will be given to you regarding weight-bearing by your physiotherapist. You are not usually allowed to take any weight through the operated side.
It is recommended for most patients that progressing from non-weight bearing to partial weight bearing with crutches will be gradual and over a period of about six weeks. If you are not able to use crutches a walking frame may be required.
While resting, it is important to keep your leg elevated to reduce swelling. Your physiotherapist will also discuss any exercises you are allowed to undertake.
You will not usually be allowed to bend your knee until after you see the surgeon at clinic.
When you go home you will wear a knee brace for up to 6 weeks.
Bowels - Bowel function can be affected by surgery and medication.
To help your bowels return to normal function you may require bowel medication.
Increasing your water intake and eating food high in fibre will also help your bowel function to return to normal. Including prunes and pear juice in your diet is recommended.
Going home - Depending on your recovery, it is anticipated you will be
discharged from day 3 after your surgery.
We aim for discharge from the ward to be 10 am.
You should have already organised your own transport home, help with meals, driving, domestic tasks, shopping and getting your compression stockings on.
Make sure the people helping you are aware of your discharge.
What complications could occur?
Serious problems from a high tibial osteotomy are not common but can happen:
- During the surgery nerves and blood vessels in the area can be damaged.
- Swelling and numbness is typical and reduces over several weeks. Compartment Syndrome can develop where the pressure within the muscles builds to a dangerous level decreasing the blood flow, nourishment and oxygen from reaching the nerves and muscles.
- Soon after the surgery people can get an infection or blood clots in their legs.
- Slippage and loosening of the plates and screws can occur.
- The bones may not unite which would require further surgery or grafting.
What can I expect from my physiotherapist?
You can contribute greatly to the success of your operation by following the intructions of your health team. It is important to consider yourself as part of the team.
Physiotherapist: While you are in hospital your physiotherapist will give information on:
- use of crutches
- getting in and out of bed
- sitting
- walking
- going up and down stairs
- getting in and out of a car.
What will it be like down the track - getting back into life!
After three months you should be back to most of your usual activities. You may
find that you can return to activities you haven’t been able to do for some time
because of your knee pain. Make the most of these improvements by getting back to
activities you enjoy.
Having prepared yourself well and participated actively in your treatment, you will be
able to return quickly to a more active independent lifestyle.
Mater Hospital Brisbane
Raymond Terrace, South Brisbane Q 4101
Telephone: 07 3163 8111

Acknowledgments
Staff of Mater Hospital Brisbane, Raymond Terrace, South Brisbane, Qld 4101
© 2010 Mater Misericordiae Ltd. ACN 096 708 922.
Mater acknowledges consumer consultation in the development of this patient information.
Mater Doc Num: PI-CLN-420021
Last modified 13/11/2018.
Consumers were consulted in the development of this patient information.
Last consumer engagement date: 11/8/2015
For further translated health information, you can visit healthtranslations.vic.gov.au/ supported by the Victorian Department of Health and Human Services that offers a range of patient information in multiple languages.